Among the most contentious issues in modern healthcare is the role of medical interventions for transgender youth—particularly the use of puberty blockers and hormone therapy for those under 18. While only about 1.6% of Americans identify as transgender or nonbinary, the number of minors pursuing gender-affirming medical care is even smaller. Yet, public opinion is starkly divided: a Pew survey found that nearly half of 10,000 respondents believe it should be illegal for healthcare professionals to provide such care to minors, and over a third think parents should be investigated for child abuse if they pursue it for their children.

Much of the media’s information consists of advocacy on either side of the issue based upon case reports – stories designed to pull on your emotional rather than analytic side. A new study in JAMA Pediatrics offers a rare glimpse into the experiences of transgender youth and their families—this time through the lens of data rather than emotion. Let's dive into the numbers and what they reveal about satisfaction, regret, and the overall impact of gender-affirming care.
The Study: Data Over Drama
The research comes from the Trans Youth Project (TYP), a long-term study that recruited participants between 2013 and 2017—individuals who had socially transitioned but had not yet begun medical treatment. In 2023, these participants (now 12 or older) and their parents were surveyed about their experiences with gender-affirming care. Of the 220 respondents, 163 were youth, and 57 were parents. The average time on puberty blockers was 4.86 years, and the average time on hormone therapy was 3.4 years. Sixty-nine additional participant data was obtained from previously identified information.
The mean age was 16.07 years, and at “last interaction,” 31% were boys, 60% were girls, and 9% were gender-diverse or nonbinary. Satisfaction and regret were assessed on a 7-point scale, reported for values between 5 and 7, above the scale midpoint.
- Overall, participants were statistically unlikely to express dissatisfaction or regret.
- Only 3% of the youth expressed dissatisfaction with puberty blockers, and 6% regretted using them. For hormone therapy, 3% were dissatisfied, and 4% expressed regret.
- 6% of parents were dissatisfied with puberty blockers, and an equal percentage regretted their use. Notably, no parents expressed dissatisfaction or regret regarding hormone therapy.
- The overwhelming majority of youth and parents felt the timing of interventions was right, with many wishing they had started earlier. Fewer than 6% believed the treatment began too soon or should never have occurred.
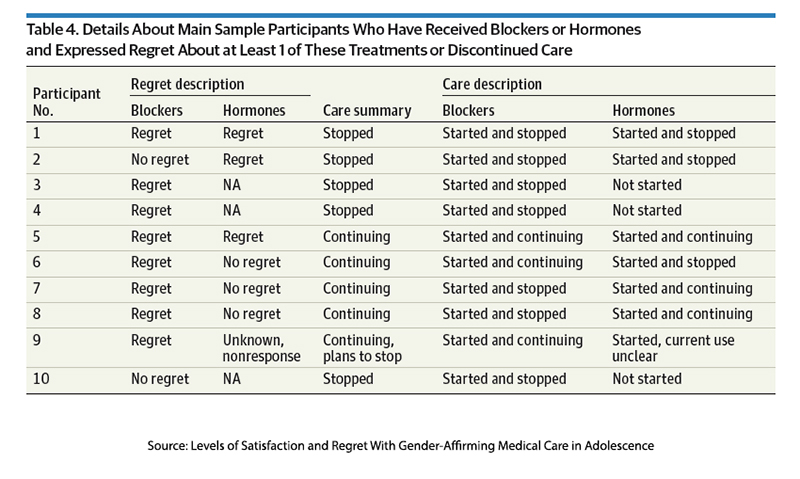
These results provide a much-needed counterpoint to the often heated and polarized debate. While regret and dissatisfaction exist, at roughly 6%, they are relatively rare. Notably, the study also found that regret, a stronger emotional response than dissatisfaction, did not necessarily lead to treatment discontinuation—half of the youth who expressed regret continued with therapy.
The researchers concluded:
“…a large cohort of early-transitioning transgender youth and their parents reported very high levels of satisfaction and low levels of regret with this care. The overwhelming majority have continued gender-affirming care.”
The greatest satisfaction for most participants came from the physical changes brought about by hormonal manipulation, while the most dislikes related to treatment administration, e.g., pain or bad experiences. While not expressed as a limitation, the researchers point out a unique feature of their cohort.
“Most showed signs of their transgender identity by 4 years of age. On average, they socially transitioned at age 6.7 years, and most were fairly binary in their gender identities and gender expressions throughout childhood. Early-identifying youth who are especially insistent about their identities are also more likely to socially transition in childhood and identify as transgender or continue to show gender dysphoria in adolescence and early adulthood. [emphasis added]
Gaining some perspective
The UK attempted to put their gender affirmative care on a more substantial, evidence-informed foundation with the Independent Review of Gender Identity Services for Children and Young People, more commonly called the Cass Review, after the study’s chairwoman, Dr. Hilary Dawn Cass, a pediatrician and former President of the Royal College of Paediatrics and Child Health. (An organization comparable to our American Academy of Pediatrics). The findings and recommendations have been controversial.
Puberty Blockers: Pausing Puberty or Time to Think?
Gonadotropin-releasing hormone (GnRH) acts within the brain's hypothalamus to control the production of sex hormones in our ovaries and testis and regulate the onset of puberty and sexual development. They were developed and tested to treat precocious puberty when a young child began the process of puberty too early. They are being used for an off-label indication, to “pause” puberty in its earliest stages in many countries to “extend the diagnostic period by buying time to think.”
As with any off-label use, the justification for their use is varied and controversial, but the majority of international guidelines cite the drug’s reversibility, the potential negative impact on bone health, and uncertainty regarding cognitive changes. Rather than a fixed age for use, most guidelines initiate treatment when the earliest signs of puberty appear. [1] The Cass Review details their meta-analysis of the efficacy of puberty blockers. Much of the report's criticism is aimed at the selection or “cherry-picking” of those studies. Leaving the scientific advocacy of both sides aside, it is clear that “puberty suppression exerts is expected physiological effect, and this has never been at issue." As the JAMA study noted, it is the source of greatest patient satisfaction.
The data reported by the Cass Review indicated that 0-8% of young people discontinued puberty suppression. They noted that in the clinic with the highest rate, 8%, the median age to initiate treatment was 15, and all were post-pubertal. The results of the JAMA study are consistent with these findings and demonstrate that discontinuation also impacts those who begin treatment far earlier.
While both JAMA and Cass identify the same 6-8% data dot, it is the subsequent narrative of the data’s meaning where advocacy bias can be seen. The JAMA study focuses on the satisfied, while the Cass Review focuses on those with regret.
“These data suggest that puberty blockers are not buying time to think…”
Masculinizing and feminizing hormones are the next stage in the trajectory of transitioning. Unlike puberty blockers, they are not used as an off-label treatment, and again, in the words of that maligned Cass Review in discussing these agents,
“for those who have undergone a successful transition, the physical costs are dramatically outweighed by the long-term benefits.”
The report takes issue with the fact that the individuals now seeking treatment differ from the older patients involved in safety studies and therapy and that no specific studies have looked at the long-term impacts of these treatments on those under age 18.
In the end, the Cass Review advised that the use of puberty blockers be continued in those already started on therapy and that their subsequent use is within clinical trials to gather more short and long-term data. They made a similar recommendation for the use of hormones in those under age 18.
“Ahead of publication of the final report NHS England took the decision to stop the routine use of puberty blockers for gender incongruence/gender dysphoria in children. NHS England and National Institute for Health and Care Research (NIHR) are establishing a clinical trial to ensure the effects of puberty blockers can be safely monitored. Within this trial, puberty blockers will be available for children with gender incongruence/ dysphoria where there is clinical agreement that the individual may benefit from taking them.”
Our political left condemned the decision “to stop the routine use of puberty blockers,” while our political right exalted that decision. Neither group emphasized that stopping referred to routine use or that treatment remained readily available within an established clinical trial.
In essence, the NHS decision is much like that of our FDA regarding post-marketing surveillance, except we do not oversee who is treated or whether adverse effects are occurring prospectively; we have an “honor” system. The UK approach differs in that all patients must participate in the research so efficacy and adverse outcomes are more readily identified, allowing an evidence-informed conversation about therapeutic trade-offs.
Dr. Cass and her work has been unnecessarily vilified and adulated. I am struck by two of her cautionary statements because she speaks as a clinician caring for patients:
“Finally, I am aware that this report will generate much discussion and that strongly held views will be expressed. While open and constructive debate is needed, I would urge everybody to remember the children and young people trying to live their lives and the families/ carers and clinicians doing their best to support them. All should be treated with compassion and respect.”
-The Cass Review
“Medicine should never be politically driven. It should be driven by evidence and ethics and shared decision-making with patients and listening to patients’ voices.” – Interview in NY Times
Gender-affirming care remains a deeply polarizing issue, but it is crucial to move beyond the emotionally charged rhetoric and focus on the data. Studies like those from *JAMA Pediatrics* and the *Cass Review* provide valuable insights into the real-world experiences of transgender youth and their families. While satisfaction rates are high, there is still room for more research and thoughtful debate to ensure that all young people receive the best possible care guided by evidence and compassion rather than politics.
In the end, the goal should be to make informed decisions that respect the individuality of each patient while continuing to gather data that can guide future generations of transgender youth.
[1] There is a well-accepted description of the stages of puberty, the Tanner Stages, that provides the criteria
Source: Levels of Satisfaction and Regret With Gender-Affirming Medical Care in Adolescence JAMA Pediatrics DOI: 10.1001/jamapediatrics.2024.4527
Americans’ Complex Views on Gender Identity and Transgender Issues Pew Research

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


